
Most denied claims are lost on process, not on the facts. If I check the payer, the product line, the deadline, and the filing path first, I cut the risk of a missed or misrouted appeal.
Here’s the short version:
- Deadlines change by payer. UHC commercial may give 65 days, while Aetna and Cigna often allow 180 days.
- The first step is not always an appeal. Some plans want a reconsideration first.
- Clinical and payment denials may go to different teams. Sending a clinical case through claims can burn time.
- BCBS is local-plan driven. I need the member’s home plan and alpha prefix for BlueCard cases.
- Medicare has a fixed 5-level path. Each level has its own clock.
- ACA and Medicaid managed care follow plan and state rules. Internal review may lead to an IRO or a state hearing.
- Appeals work more often than many teams think. About 50% to 60% of appealed denials are overturned, yet fewer than 1% of denied claims get appealed.
If I want a simple way to handle denials, I use this order:
- Identify the payer and plan type
- Confirm the deadline from the notice date
- Split the case into payment or clinical
- Send it through the right portal or address
- Save proof of submission and follow up in 7 to 10 business days
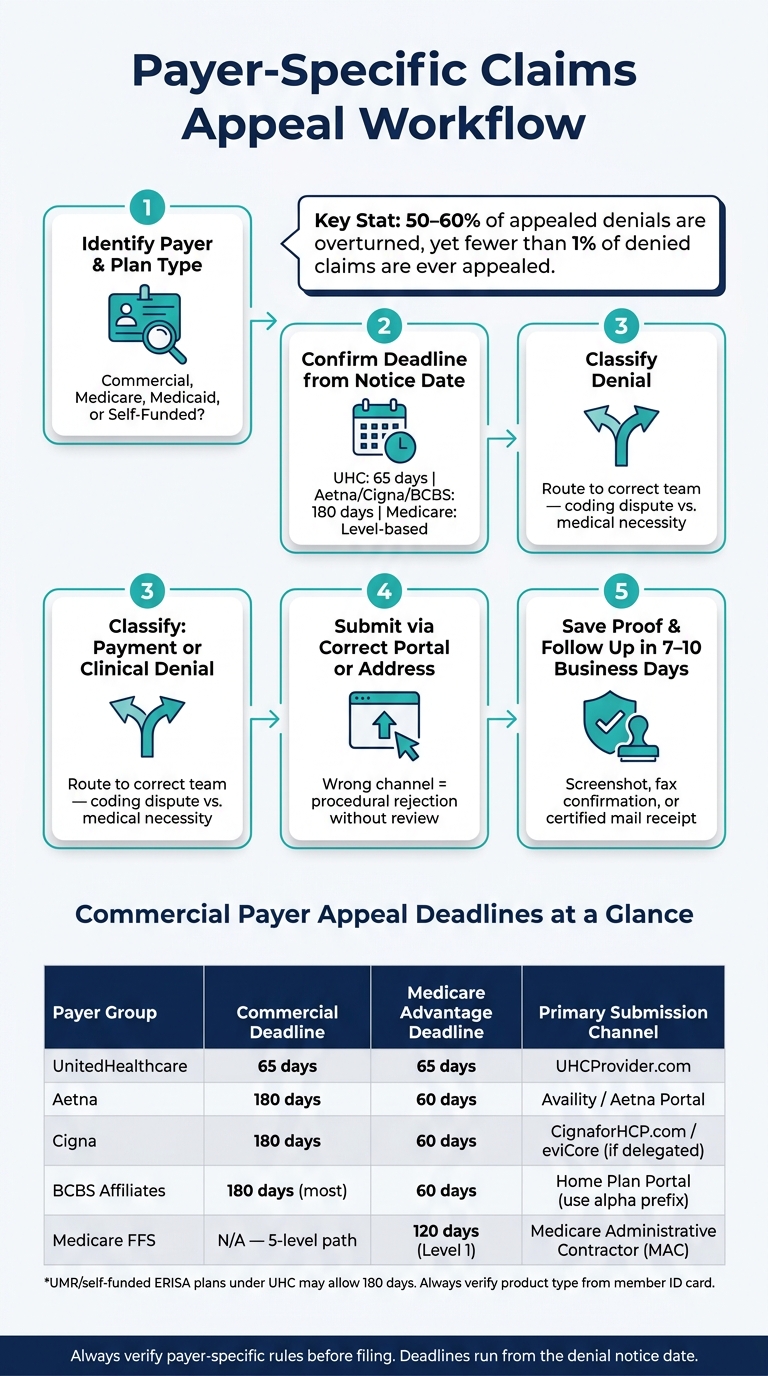
Payer-Specific Claims Appeal Workflow: 5 Steps to Avoid Denied Claims
Quick comparison
| Payer group | Common commercial window | Medicare Advantage window | Main filing point |
|---|---|---|---|
| UnitedHealthcare | 65 days | 65 days | UHC provider portal |
| Aetna | 180 days | 60 days | Availity / Aetna portal |
| Cigna | 180 days | 60 days | Cigna portal / eviCore if delegated |
| BCBS affiliates | Often 180 days | 60 days or plan rule | Home plan portal |
| Medicare FFS | Level-based | N/A | MAC |
I read this article as a playbook for one thing: match each denial to the right payer rule set before I file anything.
sbb-itb-02f5876
Major Commercial Payer Appeal Requirements
Commercial payers tend to vary in three places: product line, deadline, and who reviews the case first. In day-to-day work, that’s the simple rule to follow: the product line tells you the filing window, the form or portal, and the first review step.
UnitedHealthcare: Reconsiderations, Appeals, and Product-Line Differences
UHC requires a reconsideration before a formal appeal. For commercial plans, the appeal window is 65 calendar days from the date printed on the denial notice.
For inpatient cases, a peer-to-peer (P2P) review usually has to be requested within 3 business days of the denial. Most network providers must submit through the UHC Provider Portal.
| UHC Product Type | Appeal Deadline | Submission Route | Key Process Detail |
|---|---|---|---|
| Commercial | 65 calendar days | UHC Provider Portal / API | 2-step process: reconsideration, then formal appeal |
| Medicare Advantage | 65 calendar days | UHC Provider Portal | CMS rules also apply |
| Medicaid Community Plan | Varies by state | State-specific portal or UHC portal | Check the state contract |
| Self-Funded (UMR) | 180 calendar days | UMR portal | ERISA rules generally use the longer window |
One detail matters a lot here: plans run through UMR are self-funded ERISA plans, so they usually use a 180-day window instead of UHC’s standard 65-day commercial deadline. That’s why the member’s ID card matters so much. Before you count days, confirm the product type, send the case through the right route, and file inside the payer’s window.
After UHC, the next big divide is payment disputes versus clinical appeals.
Aetna and Cigna: Payment Disputes, Clinical Appeals, and Documentation Rules
Aetna splits payment disputes from clinical appeals. Cigna, by contrast, uses a mostly single-level internal appeal process, and its informal phone reconsideration does not use formal appeal rights.
Start by checking delegation. If the service was delegated to eviCore - often for radiology, oncology, and musculoskeletal care - the appeal has to go through the eviCore portal, not Cigna directly.
| Feature | Aetna | Cigna |
|---|---|---|
| Commercial Deadline | 180 days | 180 days |
| MA Deadline | 60 days | 60 days |
| Dispute Types | Payment dispute vs. clinical appeal | Single-level internal appeal |
| Informal Option | No informal pre-appeal step | Phone reconsideration (2 business days) |
| Primary Submission | Availity portal | CignaforHCP.com or eviCore (if delegated) |
| Required Documentation | Clinical records, claim, and EOB/PRA | Narrative, op report, and records |
If the payer misses its deadline, internal review is deemed exhausted under 29 CFR 2560.503-1. So the same basic habit still applies: verify the product type, route the case the right way, and file inside the payer’s time limit.
BCBS works a different way. The affiliate, not the brand name, controls the appeal path.
Blue Cross Blue Shield Plans: Regional Variation Under One Brand
BCBS consists of 34 independent affiliates, so appeal rules depend on the home plan. For BlueCard cases, use the member’s alpha prefix to route the appeal to the home plan, not the local host plan.
| BCBS Plan Pattern | Filing Rule | Deadline |
|---|---|---|
| Most Commercial Affiliates | Follow the home plan's manual and portal | 180 days |
| Medicare Advantage | Follow CMS requirements and the affiliate's process | 60 days minimum |
| BlueCard (Out-of-State Care) | File with the member's Home Plan using the alpha prefix | Home plan deadline applies |
The key point is simple: use the home-plan manual, because each affiliate sets its own forms and portals. Check the product type, route the case to the right plan, and file within that payer’s window.
Federal and Regulated Plan Appeals
After commercial payer variation, federal and regulated plans move through set appeal tracks. The rules are fixed. The deadlines come from regulation. Miss one step, and the appeal can stop right there.
Medicare Fee-for-Service: The 5 Appeal Levels
Medicare Parts A and B use a five-level appeal path. Each level has its own reviewer, filing method, and deadline. The path starts with the Medicare Administrative Contractor (MAC) and can end in federal court.
| Appeal Level | Adjudicator | Filing Deadline | Amount in Controversy |
|---|---|---|---|
| 1. Redetermination | MAC | Date on MSN | N/A |
| 2. Reconsideration | QIC | 180 days from Level 1 decision | N/A |
| 3. ALJ Hearing | OMHA | 60 days from Level 2 decision | $200 |
| 4. Appeals Council | Appeals Council | 60 days from Level 3 decision | N/A |
| 5. Judicial Review | Federal district court | 60 days from Level 4 decision | $1,960 |
A small detail at Level 1 can trip people up: the clock starts from the MSN date, not the day the notice shows up in the mail. So when the MSN arrives, log the printed date right away.
At Level 3, you can combine related denials for the same beneficiary to meet the $200 amount-in-controversy rule. For 2026, the Level 5 threshold for judicial review is $1,960.
There’s another rule worth flagging. If OMHA or the Appeals Council misses its decision deadline, you can move the case to the next level instead of waiting around.
ACA Marketplace Plans and Medicaid Managed Care: Internal Appeals and External Review

Outside Medicare, the first thing to sort out is the plan type. That tells you where the appeal goes next. In plain terms, does the case end in external review, or does it head to a state hearing?
For ACA Marketplace plans, if the internal appeal is denied, the case moves to an Independent Review Organization (IRO) for a final, binding decision. When the denial involves emergency services, document the patient’s presenting symptoms, not just the final diagnosis. That point matters because federal law uses the prudent layperson standard. Coverage depends on what a prudent layperson would have believed when the patient arrived, not what the diagnosis turned out to be.
Medicaid managed care often adds a state fair hearing. State law controls the last review step, which means the process can change from state to state. If the payer misses the internal appeal deadline, treat it as a deemed denial and move to external review.
| Feature | Medicare FFS | ACA Marketplace Plans | Medicaid Managed Care |
|---|---|---|---|
| Appeal Path | 5 levels: MAC, QIC, ALJ, Appeals Council, federal court | Typically 1–2 internal appeals plus external review | Internal appeal plus state fair hearing/external review |
| Common Filing Window | Level 1: MSN date; Level 2: 180 days from Level 1 decision | 60–180 days, depending on plan/state | Varies by state |
| Final Review Body | Federal district court | IRO or state agency | State fair hearing or state agency/IRO |
| Expedited Option | Available for certain Part A service terminations | 72-hour turnaround for urgent cases | 72-hour turnaround for urgent cases |
Build these fixed paths into your appeal checklist and deadline tracker.
How to Build a Payer-Specific Appeal Workflow in Your Practice
Once you've mapped each payer's rules, the next step is turning that information into a process your team can use every single time a denial shows up. Knowing the rules matters. But if the workflow falls apart in practice, denials slip through the cracks.
A Standard Appeal Checklist That Adapts to Each Payer
Start with a core appeal package that works across payers, then layer in each payer's extra requirements. In most cases, every package should include the denial notice, the original claim with patient and claim identifiers, chart notes, treatment history, and a denial-specific narrative that speaks directly to the payer's reason code.
For clinical denials, be specific. Cite the payer policy tied to the denial and point to the exact criteria the patient meets. A Physician Letter of Medical Necessity that names the precise policy section carries much more weight than a broad statement. Include failed conservative treatment, relevant imaging, and peer-reviewed guidelines only when they make the medical necessity case stronger.
It also helps to split denials into payment and clinical tracks right away. That simple step sends each denial to the right owner and keeps a coding dispute from getting stuck in the clinical appeal path.
Before anything is filed, log the deadline and the proof of submission.
Deadline Tracking, Follow-Up Cadence, and Audit Trails
Track each denial from intake through submission in one workflow log. Then track each payer's filing window from the denial date in one deadline log. That may sound basic, but this is where many teams get burned.
Log every denial as soon as it arrives. Record:
- The notice date
- The calculated filing deadline
- The submission date
- The confirmation number or fax receipt
For portal submissions, save a screenshot with the timestamp. For fax or mail, keep the fax confirmation or send it by certified mail with a return receipt.
Set a follow-up reminder for 7–10 business days after submission so your team can confirm receipt.
A HIPAA-compliant platform like Prospyr can keep records, communication logs, tasks, and timestamps in one place. That gives you a defensible audit trail if a payer asks for proof of submission and follow-up.
Common Mistakes That Lead to Avoidable Denials or Failed Appeals
The biggest problems usually come from process breakdowns, not clinical judgment. If a service is delegated, send it to the vendor's portal and appeals address, not the payer's standard channel. Send it to the wrong place, and you'll often get a procedural rejection without any review of the case itself.
Another common problem is skipping a required reconsideration step before filing a formal appeal. For Anthem, payment and coding disputes follow a two-step process, and missing Step 1 can cause you to lose Step 2 rights.
Peer-to-peer review should also be built into the clinical track early, before the written appeal goes out.
Conclusion: A Quick-Reference Framework for Payer-Specific Appeals
Every appeal starts with two basic questions: Which payer is responsible? And which product line applies? Those two details drive everything else, including the deadline, submission channel, required steps, and supporting records. Get either one wrong, and the appeal can fail before anyone even reviews it.
After that, the path is pretty simple: send the denial to the right place, file within the deadline, and document each step. Keep reconsiderations separate from appeals, route by denial type, match your records to the payer policy that was cited, and log every action with a timestamp.
Use this as a quick filing shortcut when a denial comes in.
| Payer Group | Commercial Deadline | Medicare Advantage Deadline | Primary Submission Channel |
|---|---|---|---|
| UnitedHealthcare | 65 days | 65 days | UHCProvider.com |
| Aetna | 180 days | 60 days | Availity / Aetna Portal |
| BCBS (Affiliates) | 180 days (most) | 60 days | Availity / Local Affiliate Portals |
| Cigna | 180 days | 60 days | Availity / eviCore (if delegated) |
| Medicare Fee-for-Service | N/A | 120 days (Level 1) | Medicare Administrative Contractor (MAC) |
FAQs
How do I know if a denial needs reconsideration or a formal appeal?
Start by reviewing the EOB or remittance advice closely. The denial code, plan type, and reviewing entity listed there tell you whether the next step is reconsideration or a formal appeal.
Many payers use a two-step process, so reconsideration often comes first. If you jump straight to an appeal, you may run into a procedural error.
For medical necessity denials, a peer-to-peer review is often the best first move before you send a written appeal.
What information should I verify before filing an appeal?
Before filing an appeal, check the deadline and submission rules on the denial notice. Those details can change based on the payer and the type of plan.
Next, pinpoint why the claim was denied and note any clinical criteria the payer used, including InterQual, AIM, or any proprietary policy numbers.
It also helps to confirm whether a peer-to-peer review is available. Then pull together the documents you'll need:
- Member ID
- Claim number
- Relevant medical records
- The correct appeal form
What proof of submission should I keep for an appeal?
Keep documentation that shows the claim was originally submitted on time, such as:
- EDI confirmation logs
- clearinghouse acknowledgments
- direct payer receipts
Don’t rely on screenshots alone. Keep full records that show the entire chain of custody in case you need an appeal, external review, or dispute.

