
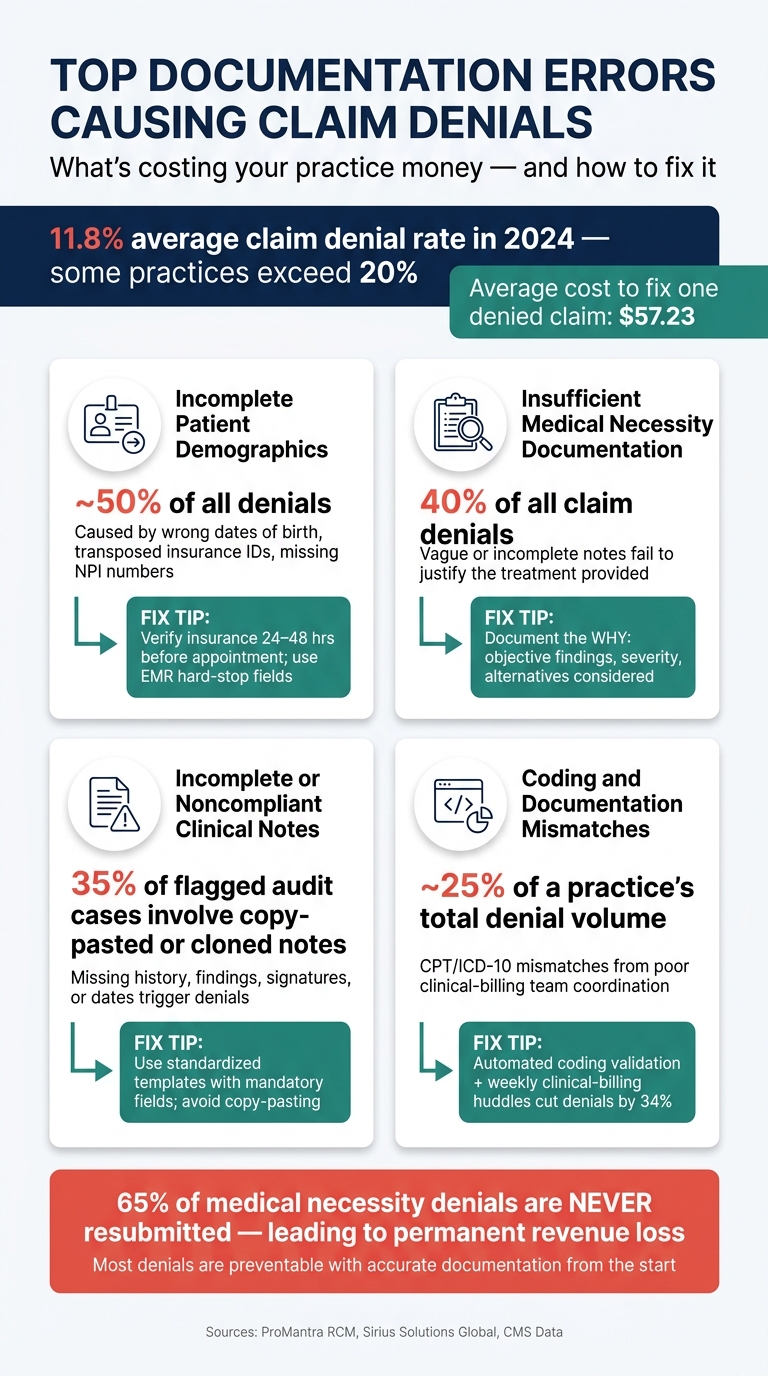
Denied claims are a major revenue drain for clinics, often caused by avoidable documentation mistakes. In 2024, denial rates for healthcare claims in the U.S. reached 11.8%, with some practices facing rates as high as 20%. Fixing a single denied claim cost an average of $57.23, and 65% of medical necessity denials were never resubmitted, leading to permanent income loss.
The most common errors include:
- Incomplete patient demographics: Wrong insurance details or missing provider information.
- Insufficient medical necessity documentation: Failing to justify treatments with clear clinical reasoning.
- Noncompliant clinical notes: Missing essential details like history, findings, or signatures.
- Coding mismatches: Errors in aligning diagnosis codes (ICD-10) with procedure codes (CPT).
To prevent these issues:
- Use digital tools to verify patient information and reduce manual errors.
- Create standardized templates with mandatory fields for complete documentation.
- Conduct regular audits to identify and fix recurring problems.
- Leverage AI-powered tools for real-time error detection and accurate note creation.
Accurate documentation is critical for reducing denials, saving time, and protecting revenue. Addressing these errors upfront ensures smoother claim submissions and better financial outcomes.
Documentation Requirements for Successful Claims
Core Documentation Standards
Every claim must clearly demonstrate the clinical need for the service provided. This means including a complete clinical note that outlines the purpose of the visit, the patient’s history, exam findings, diagnostic test results, assessment, treatment plan, date, and provider identity. If any of these elements are missing, the claim risks being denied.
It’s equally important to ensure that ICD-10 diagnosis codes and CPT procedure codes align logically. Any mismatch between these can lead to an automatic rejection. As ProMantra RCM explains:
"Clinical necessity and documented necessity are two different things. If the patient genuinely needed the service but the documentation doesn't clearly prove it by payer standards, the claim can still be denied."
By mastering these documentation standards, you can better understand and prevent common claim denials.
Common Types of Claim Denials
Not all denials are created equal, and the way you respond depends on the type of denial. Claims can fall into two main categories: soft denials and hard denials.
| Denial Type | What It Means | Can It Be Reversed? |
|---|---|---|
| Soft Denial | Minor technical issues like a missing signature, incorrect code, or incomplete data | Yes, if corrected promptly |
| Hard Denial | Clinical issues, such as failing to meet medical necessity criteria | Requires a formal appeal and is much harder to overturn |
Shockingly, 65% of medical necessity denials are never resubmitted. This highlights the importance of accurate documentation upfront. Preventing hard denials is far more effective than trying to appeal them later.
How Payers Classify Aesthetic and Wellness Services
Payers make a clear distinction between cosmetic procedures and those deemed medically necessary. Your documentation plays a crucial role in determining how a claim is classified. Leading insurers like UnitedHealthcare, Cigna, and Aetna now rely on algorithmic tools and Natural Language Processing (NLP) to analyze clinical notes for specific keywords before a human reviewer even looks at the claim. Using vague or cosmetic-sounding terms can lead to automatic reclassification as a cosmetic procedure. Instead, focus on documenting clinical findings such as "chronic irritation," "bleeding on contact," or "restricted range of motion."
Here’s how documentation can make or break coverage for common procedures:
| Procedure | Payer's Default Classification | What Your Notes Must Show |
|---|---|---|
| Botox Injection | Wrinkle reduction (cosmetic) | Conditions like hyperhidrosis (R61.1) or chronic migraines (G43.909) |
| Laser Treatment | Skin rejuvenation (cosmetic) | Actinic keratosis (L57.0) or vascular lesions with functional impact |
| Scar Revision | Aesthetic improvement (cosmetic) | Hypertrophic scars (L91.0) causing pain or functional limitations |
| Lesion Removal | Appearance improvement (cosmetic) | Evidence of chronic irritation, bleeding, or recurrent infections |
Avoid documenting phrases like "subjective dissatisfaction" as they can automatically shift the claim into cosmetic territory. Instead, emphasize functional impairments, such as pain severity, recurrent infections, or limitations in daily activities. This type of precise documentation helps ensure that payers classify the procedure as medically necessary.
sbb-itb-02f5876
Top Documentation Errors That Cause Claim Denials
Top Documentation Errors Causing Claim Denials: Key Stats
Claim denials can lead to significant revenue loss, and understanding the common reasons behind them is key to avoiding these setbacks. In 2026, denial rates reached 12%–14%, with poorly documented practices seeing rates climb above 20%. These errors not only delay payments but also create extra work for clinicians and billing teams. Let’s break down the most frequent documentation mistakes and how to address them effectively.
Incomplete Patient Demographics and Insurance Information
Errors made during the patient intake process are one of the most preventable causes of claim denials. Mistakes like entering an incorrect date of birth, transposing an insurance ID number, using an outdated group number, or omitting the provider’s NPI can lead to automatic rejections. These front-end issues account for nearly 50% of all denials.
To reduce these errors:
- Verify insurance details during scheduling and again 24–48 hours before the appointment.
- Use digital intake forms to minimize manual input errors.
- Implement EMR systems with hard-stop fields to ensure all required information is entered.
Fixing these errors early in the process saves time and prevents unnecessary revenue loss.
Insufficient Medical Necessity Documentation
Medical necessity issues are responsible for 40% of all claim denials, making them one of the most costly documentation problems. The problem often isn’t that the service wasn’t necessary - it’s that the documentation doesn’t clearly demonstrate the need. Vague or incomplete entries fail to justify the treatment provided.
"Your clinical skills mean nothing to insurance companies if you cannot prove what you did." - Sirius Solutions Global
To avoid these denials, focus on documenting the why, not just the what. Include:
- Objective findings and condition severity.
- Alternative treatments considered.
- A clear connection between the diagnosis and the procedure performed.
EMR templates with mandatory fields for medical necessity rationale can help ensure all critical details are captured.
Incomplete or Noncompliant Clinical Notes
Clinical notes that lack essential elements - such as a complete history, objective findings, treatment plan, provider identity, or date of service - are a common reason for denials. Additionally, cloned or copy-pasted notes raise red flags for payers and auditors, as they suggest care isn't being tailored to the individual patient.
To improve compliance:
- Use standardized templates with required fields to ensure all necessary information is included.
- Consider AI-assisted tools that help providers create accurate and complete notes in real time, reducing the need to reconstruct details later.
Coding and Documentation Mismatches
Coding errors are another major driver of claim denials, accounting for about 25% of a practice's total denial volume. These errors often stem from a lack of coordination between clinical and billing teams, leading to unsupported CPT codes.
"Most upcoding issues are unintentional, happening because of poor communication between clinical and billing staff." - Sirius Solutions Global
To address this issue:
- Use automated coding validation tools to check CPT/ICD-10 combinations against NCCI edits before submission.
- Hold brief, weekly huddles between clinicians and billing managers to review recent denials and identify gaps. One practice reduced documentation-related denials by 34% within two months after adopting this approach.
How to Build Better Documentation Processes
Spotting documentation errors is just the beginning; the real challenge lies in stopping them from happening in the first place.
Standardized Documentation Workflows
One way to minimize denials is by making thorough documentation the easiest option. This involves creating templates with mandatory fields - like diagnosis, medical necessity rationale, treatment plan, and provider signature - so critical details aren't overlooked. For example, if a provider can't finalize a note without linking the diagnosis to the treatment, the note is far more likely to be accurate.
Real-time clinical prompts can take this approach further. Templates that require providers to explain their treatment choices and include objective findings supporting their diagnosis address the kind of clinical reasoning payers expect. Add EMR hard stops to prevent finalizing notes until all required fields are completed, and you've tackled many technical denials before they even reach a payer.
"Documentation quality is not just a clinical requirement - it is a direct driver of financial performance." - Ameridial
It's worth noting that Medicare standards don't always align with commercial payer requirements. To stay compliant, regularly update workflows as payer policies evolve, such as those outlined in CMS-0057-F.
While standardized workflows are essential, their effectiveness depends on regular audits to ensure they remain on track.
Internal Audits and Staff Feedback
Creating better workflows is only part of the solution - continuous monitoring is just as important. Regular internal audits act as an early detection system. Conduct monthly reviews of documentation completeness by randomly sampling 5–10 charts, and for new providers, perform targeted audits every 30 days during their first 90 days to address issues early on.
Audit data often highlights recurring problems. Common issues include repetitive or copy-pasted notes (35% of flagged cases), incomplete or missing History of Present Illness (28%), and diagnoses that aren't backed by the documentation (24%). Sharing these findings with staff using real-world denial examples - not just abstract rules - makes training sessions more practical and impactful.
CMS has been ramping up its audit efforts, increasing the number of Medicare Advantage plans reviewed from 60 to 550 and the records examined from 35 to 200. Waiting for external audits to reveal gaps can lead to major compliance risks.
Using Technology to Reduce Documentation Errors
Technology, when integrated with standardized workflows and regular audits, can significantly cut down on documentation mistakes. Real-time validation tools embedded in workflows catch errors as they happen. Tools like automated validation systems, digital intake forms, and AI-powered note creation - such as those offered by Prospyr - are shown to reduce denials by up to 40% and speed up reimbursements by 30%.
For aesthetics and wellness clinics, Prospyr addresses documentation risks at multiple stages of the patient journey. Digital intake forms help eliminate manual entry errors upfront, while integrated CRM/EMR tools and AI note creation ensure providers capture complete and accurate clinical data during patient visits. Automated audit trails log every action with timestamps, offering clarity during both internal and external audits without adding extra work for the clinical team.
The aim isn't to replace clinical judgment with technology but to ensure that judgment is consistently and thoroughly documented every time. By combining robust workflows, ongoing audits, and smart technology, practices can significantly improve their documentation processes.
Conclusion
Documentation errors don’t just make administrative tasks harder - they can also hurt your bottom line. High denial rates and lost claims are ongoing issues for practices that fail to prioritize documentation quality.
The good news? Most denials are avoidable. Issues like vague clinical notes, unsupported medical necessity, coding errors, missing signatures, and overused copy-pasting can all be addressed with accurate and thorough documentation from the beginning.
Creating better documentation requires structured workflows, regular audits, and the right technology. For aesthetics and wellness clinics, tools like Prospyr offer solutions such as digital intake forms, AI-assisted note creation, and CRM/EMR integration. These features ensure that critical details aren’t overlooked during patient visits, linking precise documentation directly to better financial performance.
FAQs
What should I document to prove medical necessity?
To establish medical necessity, it's essential to clearly outline the clinical indication, provide evidence of any prior conservative treatments (if relevant), and explain the expected benefit of the service. Be sure to include objective findings, a detailed timeline of symptoms, and how the service will impact diagnosis or treatment decisions. Well-organized and detailed documentation not only strengthens claims but also helps minimize the chances of denials.
How can I stop demographic and insurance errors at intake?
To cut down on errors during patient intake, make sure to confirm key details, such as the patient’s legal name, date of birth, address, and insurance ID, right before their appointment. Digital intake forms can be a big help here, allowing patients to review and update their information ahead of time. Adding real-time insurance verification to your process and cross-checking details with the physical insurance card can also reduce mistakes. Additionally, training your staff to follow standardized data entry practices and use templates can go a long way in avoiding errors that might lead to claim denials.
How do I avoid “cosmetic” wording that triggers denials?
To avoid claim denials tied to "cosmetic" wording, make sure your documentation highlights medical necessity. Be thorough by detailing specific symptoms, the clinical reasoning behind the procedure, prior conservative treatments attempted, and measurable indicators of severity. Stay away from vague or speculative language that might imply a non-medical purpose.

