
If I had to boil this down to one line, it’s this: ICD-10-CM tells why the patient is there, and CPT tells what I did.
That single split drives coding for cosmetic consults, self-pay visits, and mixed cosmetic/medical cases. In this article, I walk through how to use Z41.1 for elective cosmetic visits, when a medical diagnosis like J34.2, N62, or H02.831–H02.834 changes the billing path, and how CPT, E/M rules, and modifiers like 25, 59, and GY fit into the same encounter.
Here’s the short version:
- Use ICD-10-CM for the reason for the visit
- Use CPT for the service performed
- Don’t code a cosmetic case as medical just to bill insurance
- If a visit is functional, the chart needs proof like visual field testing, imaging, or failed prior treatment —all of which can be captured during digital intake to streamline the workflow.
- Same-day E/M plus procedure may need Modifier 25
- Missing documentation can lead to denials, especially for excisions and mixed medical/cosmetic visits
- Keep code sets current every year to avoid claim problems
A simple example:
- Pure cosmetic facelift consult/procedure: ICD-10-CM Z41.1
- Service performed: CPT code tied to the actual procedure, such as 15824 in the article’s example
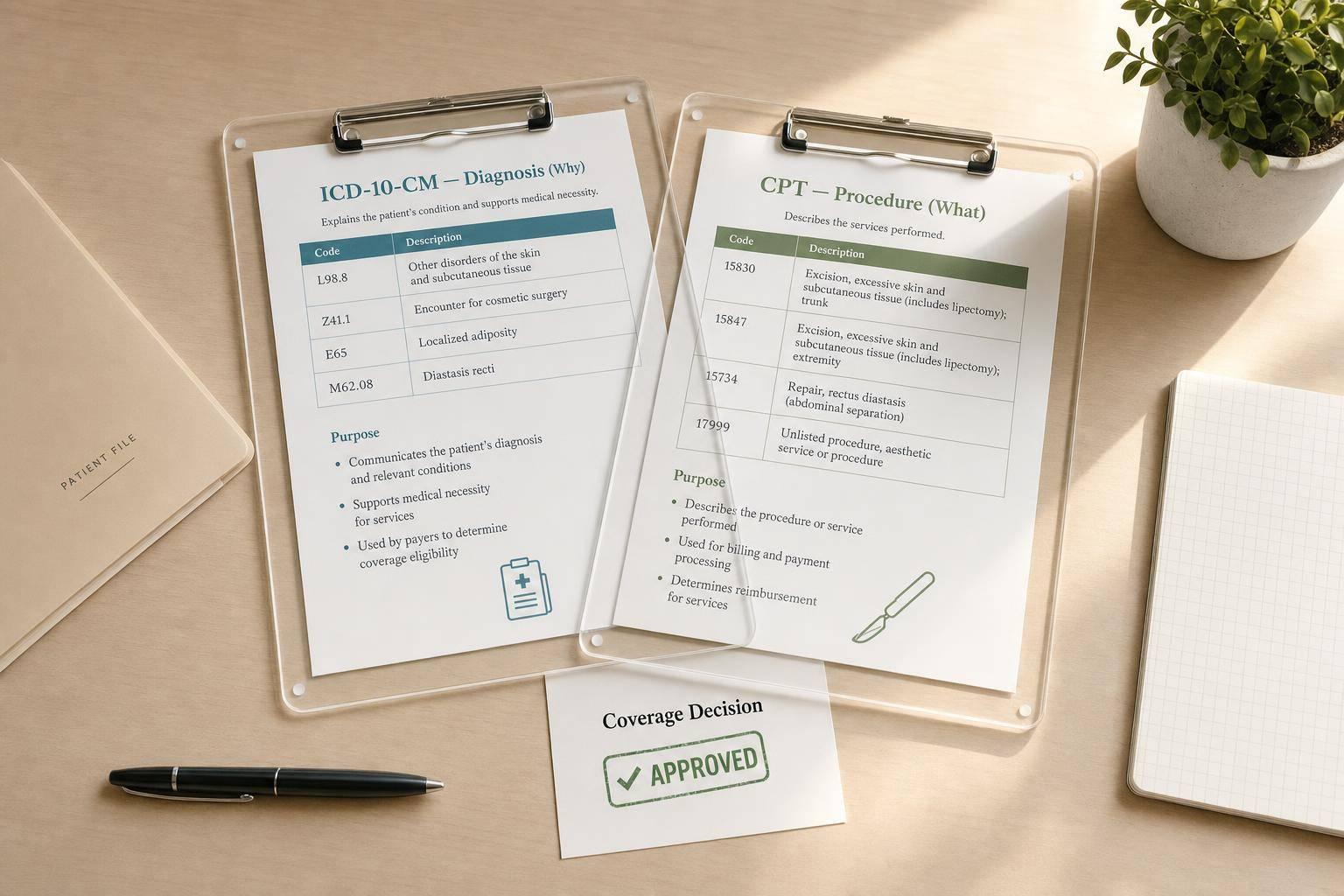
Quick Comparison
| Code Set | What it answers | Cosmetic example | Main billing role |
|---|---|---|---|
| ICD-10-CM | Why did the patient come in? | Z41.1 | Shows whether the visit is elective or tied to a functional diagnosis |
| CPT | What did I do? | 15823, 15824, or an E/M code when supported | Shows the visit, procedure, or both |
I wrote this summary to make one point clear: clean cosmetic billing starts with matching the diagnosis to the service and backing both with the chart.
sbb-itb-02f5876
ICD Codes in Cosmetic Consultations
In a cosmetic consultation, ICD-10-CM shows the clinical reason for the visit. It also helps show whether the encounter is purely elective or tied to a medical issue.
What ICD-10-CM Documents in an Aesthetic Visit
For a visit that is cosmetic only, the standard primary code is Z41.1 (Encounter for cosmetic surgery). This code marks the encounter as elective.
One key point: Z41.1 should not be paired with Z42.- for the same condition. The Z42 series is used for plastic and reconstructive surgery after a medical procedure or a healed injury.
How Diagnosis Coding Affects Medical Necessity Decisions
Diagnosis coding matters most when a procedure can fall into either bucket: cosmetic or functional.
Take blepharoplasty. It may be done for appearance alone, or it may treat dermatochalasis (H02.831–H02.834) that blocks the visual field. The same goes for rhinoplasty. In some cases, it corrects a deviated septum (J34.2) that leads to nasal obstruction.
When the visit supports a functional diagnosis, the chart needs objective proof, such as:
- Visual field testing
- Imaging
- Documented failed conservative treatment
That’s what separates an elective cosmetic case from treatment driven by function or symptoms.
| Condition / Purpose | ICD-10-CM Code | Clinical Context |
|---|---|---|
| Elective cosmetic surgery | Z41.1 | Standard code for purely aesthetic encounters |
| Deviated nasal septum | J34.2 | Functional septorhinoplasty |
| Hypertrophy of breast (macromastia) | N62 | Medically necessary breast reduction |
| Dermatochalasis (eyelid) | H02.831–H02.834 | Functional blepharoplasty with visual field obstruction |
Once the diagnosis is set, CPT captures the service performed.
CPT Codes in Cosmetic Consultations
Once ICD-10-CM explains the diagnosis, CPT shows what the provider did during the visit. In a cosmetic consultation, that usually comes down to one issue: is the visit billed as an evaluation, a procedure, or both?
E/M and Procedure Coding Basics
You should bill an E/M code only when the consult is separately documented and backed by medical decision-making or time. So yes, CPT can apply to a consult even if no treatment happens that day.
Common procedure code examples include lesion excisions, chemodenervation, and unlisted procedures when no specific code fits.
Modifiers, Non-Covered Services, and Documentation Standards
Even when the patient pays out of pocket, cosmetic services still need CPT coding for tracking, agreements, and audit support.
If the provider performs both an E/M service and a procedure on the same day, add Modifier 25 to the E/M code. This shows the visit was a significant, separately identifiable service.
For noncovered Medicare cosmetic services, append GY after obtaining an ABN.
CPT choice also needs to line up with the chart. For excision codes, the record must include three measurements:
- Lesion diameter
- Surgical margins
- Final excised diameter
Leave out even one, and the claim is much more likely to be denied.
| Modifier | When to Use It | Common Scenario |
|---|---|---|
| 25 | Significant, separately identifiable E/M on the same day as a procedure | Consultation followed by same-day Botox or biopsy |
| 59 | Separate procedure at a different site | Two separate procedures at different anatomical sites |
| GY | Service statutorily excluded from Medicare coverage | Cosmetic procedure billed to Medicare to generate a denial |
That’s what makes the ICD and CPT comparison useful in the same encounter.
ICD vs. CPT: Key Differences and How They Work Together
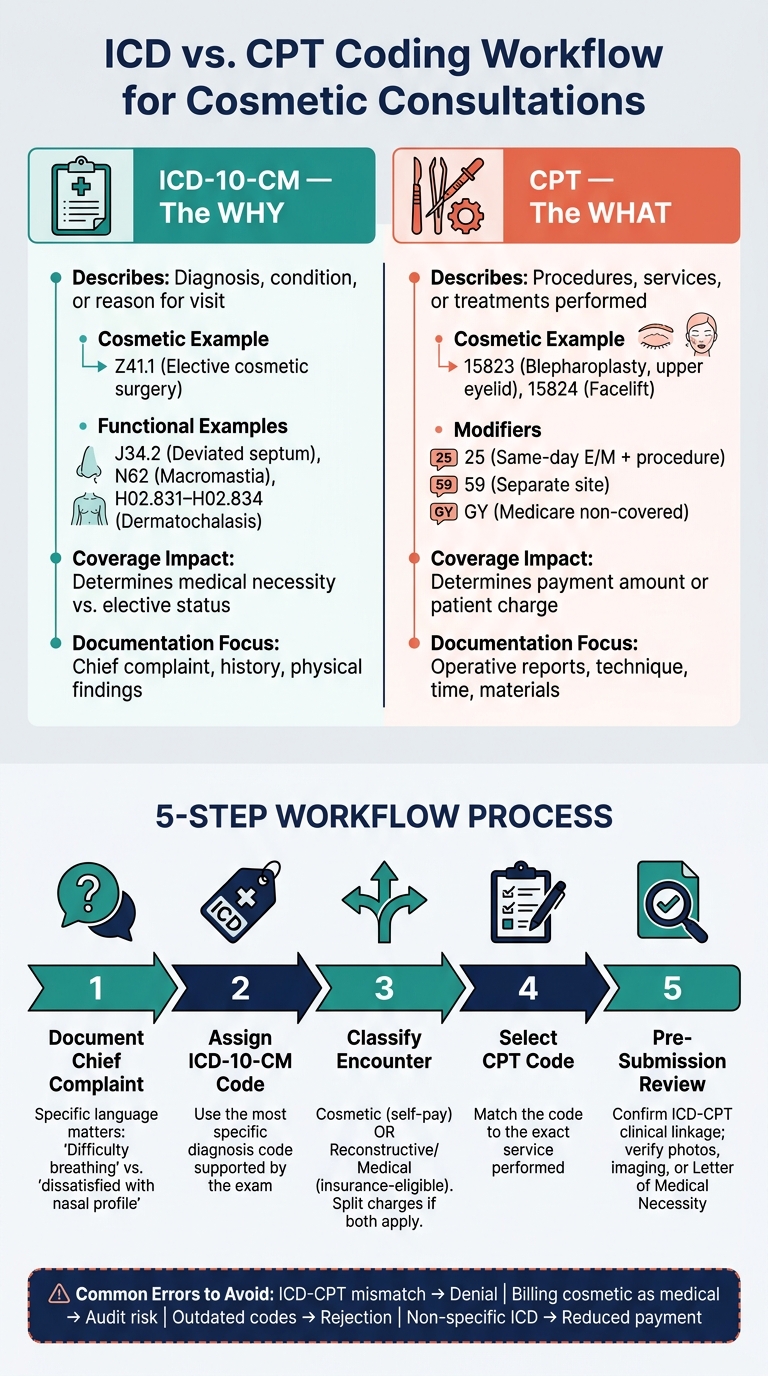
ICD vs. CPT Coding Workflow for Cosmetic Consultations
Once you separate the two code sets, the next step is simple: do they fit the same visit? ICD-10-CM explains the diagnosis. CPT explains the service. Put together, they connect why the patient came in with what was done.
ICD and CPT Side-by-Side: A Comparison Table for Cosmetic Practices
Use the comparison below to see how these code sets differ during a cosmetic consult.
| Feature | ICD-10-CM | CPT |
|---|---|---|
| What It Describes | Diagnosis, condition, or reason for visit ("the why") | Procedures, services, or treatments performed ("the what") |
| Cosmetic Example | Z41.1 (Encounter for cosmetic surgery) | 15823 (Blepharoplasty, upper eyelid) |
| Coverage impact | Determines whether the service is medically necessary or elective | Determines the payment amount or patient charge |
| Documentation focus | Chief complaint, history, physical findings, and diagnosis | Operative reports, technique used, time spent, and materials |
Common Coding Mistakes in Cosmetic Consultations
The biggest billing problem is usually a mismatch. If the ICD code does not logically support the CPT code, payers may deny the claim or flag it for review. That’s where a clean workflow helps.
| Common Error | Likely Consequence | Prevention Step |
|---|---|---|
| ICD-CPT mismatch | Claim denial for lack of medical necessity | Confirm the diagnosis code specifically supports the procedure, such as a deviated septum (J34.2) supporting septoplasty |
| Billing cosmetic as medical | Audit risk and recoupments | Never attach a medical diagnosis code to a purely elective procedure to push it through insurance |
| Non-specific ICD codes | Reduced payment or outright rejection | Use the most detailed code available; avoid "unspecified" when a precise diagnosis is documented |
| E/M note does not support the level billed | Downcoding or denial | Tie the note to time or medical decision-making |
| Outdated code libraries | Claim denials | Keep code sets current with annual AMA and CMS updates |
Bill the functional diagnosis, not the cosmetic goal.
A Simple Workflow for Using Both Code Sets on One Visit
After coding each side on its own, match them before submission.
- Intake and chief complaint: Streamline this step with online scheduling tools that capture patient data early. Document the patient’s main reason for the visit in clear, specific terms. “Difficulty breathing” tells a payer something very different from “dissatisfied with nasal profile”.
- ICD coding: Assign the most specific ICD-10-CM code supported by the exam.
- Status determination: Clearly label the encounter as cosmetic (self-pay) or reconstructive/medical (insurance-eligible). If both apply, split the charting and charges.
- CPT selection: Choose the CPT code that matches the service performed.
- Final chart review: Before submitting the claim or creating a patient invoice, make sure the ICD and CPT codes are clinically linked and that the documentation - photos, imaging, or a Letter of Medical Necessity - backs up that link. This step helps catch mismatches before submission.
Conclusion: Build a Cleaner Cosmetic Consultation Workflow
The last check is simple, but it carries a lot of weight: why did the patient come in, and what service was performed? ICD-10-CM answers the first question. CPT answers the second. When those two pieces line up, billing is easier to support for self-pay visits, insurance claims, and audit review.
In practice, the workflow should stay the same every time: document the complaint, code the diagnosis, classify the encounter, and then match the CPT code to the service. That step-by-step process gives your team a clear path instead of leaving things to guesswork.
As patient volume grows, consistency has to come from systems, not memory. Software like Prospyr can help keep that flow in place by connecting intake, charting, and billing in one HIPAA-compliant workflow. That can cut down on ICD-CPT mismatches before a claim goes out. And that matters, because code linkage is a clinical decision, not clerical busywork.
Key Takeaways
- ICD-10-CM explains why; CPT explains what.
- Cosmetic vs. reconstructive classification decides whether a service is self-pay or may qualify for insurance.
- Use documentation-first coding and a repeatable pre-submission check to cut denials, audit risk, and revenue leakage.
- Keep code sets current with annual AMA and CMS updates to avoid claim denials tied to outdated codes.
FAQs
When should I use Z41.1 instead of a medical diagnosis code?
Use ICD-10 code Z41.1 only when the procedure is strictly cosmetic and not medically necessary. This code tells payers the service is excluded from coverage.
Don’t use a medical diagnosis code for a cosmetic procedure. Doing that can trigger billing fraud concerns. If a patient still wants to submit a claim, use Z41.1 with a -GY modifier so the denial is handled transparently.
Can a cosmetic consultation be billed to insurance?
Usually, no. If the consultation is solely cosmetic, insurance doesn’t cover it, so the provider should collect payment directly from the patient.
It may be reimbursable only when there’s documented medical necessity, such as correcting a functional impairment. In those cases, the documentation needs to clearly link the procedure codes to a specific medical diagnosis.
What documentation is needed for a mixed cosmetic and medical visit?
Documentation needs to clearly separate the clinical reason for each service. That helps support accurate coding and can prevent audit problems down the line. Every encounter should also include legible records, the patient’s identification, and the practitioner’s signature.
Each billed service must have a CPT code and a matching ICD-10-CM diagnosis code. If a procedure could be seen as cosmetic or medical, include detailed operative notes. It also helps to use the right modifiers or waivers when a service isn’t covered.

